Dr Chris was invited to present a poster : “Chest X-ray Findings on 139 Hypoxic Children at High Altitude” in the Peaks District three hours north of London. She also gave a presentation with slides to the assembly of over 200 doctors from around the world-Japan to Kyrgyzstan. She introduced our book “Surviving and Thriving at Altitude” in the section on mountain literature and addressed a small group with an overview of conditions she sees in children at altitude. The meeting was held in a tent with the participants in their puffy jackets carrying their backpacks.
Speakers covered topics relevant to mountain living including “Women at Altitude”, “Children at Altitude”, hypoxic training for athletes, REDs: relative energy deficiency syndrome, climate change, hypothermia, frostbite, and more.
A concern here in Colorado with so many world class athletes, especially adolescents, is the balance between calories burned and calories needed for maximum muscle development and performance. REDs affects every system in the body, from sleep to mental and physical well-being. German orthopedic and trauma surgeon Volker Schoffl works with Olympic athletes using a questionnaire for initial screening, blood tests and physical exam to establish the diagnosis. A team of psychologists, nutritionists and physicians determine and implement treatment.
Experts from The Altitude Centre in London, James Barber and Dr. Patrycja Jonetzko, a cardiothoracic anesthesiologist, described programs to prepare athletes competing in low oxygen environments. Using equipment to create a hypoxic environment such as face masks and tents, they expose subjects for various lengths of time from minutes to hours during the weeks leading to the event. They described progress towards individualized targeted programs to increase mitochondrial efficiency.
Physiology of altitude adjustment
Dr Deborah Miller spoke during the section on “Children at Altitude” . She had just spent three months working as a pediatrician in Saipan in Micronesia where we first met. Her altitude expertise comes not only from several rotations in remote mountain clinics but personal experience with altitude illness in her children in Nepal and Colorado. She described her experience at the HRA Clinic in Nepal, at 14,300 ft. Her talk included environmental exposures with descriptions of sun toxicity. Ultraviolet radiation exposure is increased by 90% due to reflection of light from snow compared to 15-30% from sand or 5-20% from water. Treatment is similar to that for hives with antihistamines and topical steroids.
Dr Miller shared guidelines for estimated walking distances with children from momgoescamping.com. Start with ½ mile per year of age, reduce by 50% for steep elevation, increase by 10% if the destination is of interest to the child and by 25-50% if they have friends along. Now for the pack: decrease distance by 10% while assuming you will end up carrying it, and another 10% if you have a heavy pack.
The final and most important points from both her and Dr. Chris’ experience about children visiting altitude are:
Previous excellent altitude performance does not always predict future performance
Recent illness can play a role (and make them more susceptible to altitude illness)
Emergency plans are important
HAPE can take a long time to fully resolve
The day devoted to frostbite and hypothermia highlighted the importance of international registries and cooperation for progress in these devastating conditions. Although Canada, Alaska and Scandinavia have many cases the group leading investigations is based in Minnesota, where extremely cold winters and homelessness create conditions that make frostbite and hypothermia common. Rachel Nygaard, PhD discussed her work in this field.
There were fascinating and complex discussions about how and when to combine the various drugs used for resuscitation from cardiac arrest in hypothermia and the vasodilators for frostbite. Of course, there was emphasis on the universal adage that “no one is dead until they are warm and dead”, citing cases of cardiac arrest for over 2 hours with full recovery.
There were many more interesting sessions and much informal learning and networking. Dr. Chris was reacquainted with physicians who remembered her presentations at conferences in Telluride in 2016, Snowbird in 2024 and Lake Louise in 2025.
You may be surprised to learn that the University of California San Diego has been on the forefront of high altitude and hypoxia research since 1968. I recently attended the 9th Annual Center for Physiologic Genomics of Low Oxygen Summit (CPGLO) led by Tatum Simonson PhD where I gave a short presentation on Growth At Altitude. I met Dr John West who joined the university in 1968 after a Mount Everest research expedition with Sir Edmund Hillary in 1960. He also consulted for NASA serving on the advisory committee for Spacelab. He studied medicine and physiology at the University of Adelaide.
Dr. Chris and Dr. John West
The featured speaker was Isha Jain PhD from the University of San Francisco. Her research on mice shows how chronic hypoxia can mitigate and possibly cure some conditions, such as the devasting condition of mitochondrial disease. Colleen Julian PhD, from the University of Colorado, gave a talk on “Surviving Birth at Altitude: Genetic and Physiologic Insights”.
Other short presentations included a scientist from Florida who spoke of studying waterfowl who migrate at very high altitude as well as diving deep into the water to fish, thus adapted to two very different low oxygen environments. Among the poster presentations were a study on the effects of hypoxia on mitochondrial function in fibroblasts from loggerhead sea turtles presented by B. Gabriela Arango from the University of California Berkeley and a study on sleep apnea in self-identified Latinos.
Gabriela Arango from University of California Berkeley with her sea turtle research poster.
Acknowledging that chronic hypoxia may increase the risk of depression and suicide, the benefits include decreased incidence of obesity and diabetes and lower cholesterol/LDL with decreased or unchanged hypertension. These scientists study animals to help us understand the effects of our environment on our health. At conferences like this, we discuss how what I see as a clinician could be related to their study on the cellular and genomic levels.
Gabriela Arango and Dr. Chris were excited to meet again after both presented at the Hypoxia 2025 conference in Lake Louise, Canada in February
Early in the pandemic, researchers were eager to learn more about the COVID-19 virus and how it takes shape in different communities. One area of particular interest for some of those researchers was the relationship between COVID-19 and high altitude, as altitude has been shown to impact other chronic diseases like COPD1, lung cancer2, and cardiovascular disease3. However, many of the early studies that were conducted resulted in nonspecific findings or trends in data that could be better explained by different variables than solely altitude.
For example, one of the preliminary studies conducted in Colombia analyzed positive cases, deaths, and case fatality rates in 70 different municipalities ranging from 1 to 3180m above sea level. What these researchers found was that there was a negative correlation between altitude and COVID-19 case fatality rates4, meaning there were less COVID-19 deaths at higher altitude when compared to those at low altitude. One thing that is mentioned by the researchers is that population density plays an important role in the transmission of this virus4. The researchers concluded that this negative correlation seen between altitude and COVID-19 fatalities could be better explained by the differences in population in the varying locations4.
Another early study conducted in 2020 looked at around 4 months of data in the U.S and around 2 months of data in Mexico and found that U.S. communities living at >2000m elevation had higher mortality rates than those at <1500m5. In Mexico, individuals <65 years old, the risk of death due to COVID-19 was 36% for those living at >2000m when compared to those living at <1500m5.
We discussed some of these findings with Dr. Isain Zapata, who is one of the authors of the article “Revisiting the COVID-19 fatality rate and altitude associated through a comprehensive analysis”. Which was a study conducted by a group of researchers at Rocky Vista University that further investigated the relationship between altitude and COVID-19 fatalities. Dr. Zapata said that some of their motivation to look further into this relationship was due to the lack of consistency in the conclusions formed by many of the studies conducted early in the pandemic. He hypothesized that there could be a few reasons for these inconsistencies, one being that there is a large discrepancy over what level of elevation is considered “high altitude” and another being that many of the studies published early on were specific to a certain location. Lastly, these studies were solely looking at data from the first few months of the pandemic, when COVID-19 infections were just beginning to take form.
In their study, this group of researchers looked at COVID-19 fatality data from March 2020 to March 2021 in the mountain region of the western United States, including Montana, Idaho, Wyoming, Nevada, Utah, Colorado, Arizona, and New Mexico. Within each state, they looked at the data specific to each county and then subdivided them into census blocks6. Then determined the weighted average of the block’s altitude and adjusted for population density6.
They found that in Colorado, Idaho, and Wyoming, communities living at higher altitude had lower COVID-19 fatality rates6. This trend was also observed when they performed a meta-analysis of all of the data from the U.S. Mountain region6. However, when looking at Arizona, Montana, Nevada, and Utah individually, there was not a significant relationship observed between high altitude and COVID-19 mortality6. One of the points discussed by the researchers is that in these states, the discrepancy may be based on the population density6. In Arizona and Nevada, the majority of the population in that state live at lower altitudes6. The researchers also discuss that the size of the state and the number of counties in each state may also play a role in these trends6.
They also found that in Arizona, Colorado, Idaho, and Wyoming, areas with higher median incomes were associated with lower COVID-19 fatality rates6.
The researchers observed that in New Mexico, there was a reverse altitude effect, in which, there was higher mortality rates at higher altitudes6. There was also a higher associated risk across the whole mountain region for the Native American population6. One observation that was pointed out in the discussion section of this article, is that New Mexico has one of the highest Native American populations6. In addition, Native Americans have been shown to have higher incidence of developing chronic diseases that are associated with worse COVID-19 fatality rates6.
So, what does this all of this mean? Overall, in the U.S. western Mountain region, there were fewer Covid-19 deaths for communities living at higher altitude when compared to those living at lower altitude6. This same trend was observed when just looking at the data for Colorado6.
Another point that was discussed by the researchers is that these implications can likely be explained by both protective physiologic changes that occur at altitude as well as demographic trends6. The demographic trend may be hypothesized to be a result of people who choose to live in areas of higher altitude as they are often seeking more active lifestyles. The results of this study leave room for more research to be conducted on how our bodies physiology changes in order to adapt to life at higher altitudes.
Andreas Horner et al., “Altitude and COPD Prevalence: Analysis of the Prepocol-Platino-Bold-Epi-Scan Study,” Respiratory Research 18, no. 1 (August 23, 2017), https://doi.org/10.1186/s12931-017-0643-5.
Kamen P. Simeonov and Daniel S. Himmelstein, Lung Cancer Incidence Decreases with Elevation: Evidence for Oxygen as an Inhaled Carcinogen, November 12, 2014, https://doi.org/10.7287/peerj.preprints.587v2.
Eder Cano-Pérez et al., “Negative Correlation between Altitude and Covid-19 Pandemic in Colombia: A Preliminary Report,” The American Journal of Tropical Medicine and Hygiene 103, no. 6 (December 2, 2020): 2347–49, https://doi.org/10.4269/ajtmh.20-1027.
Orison O. Woolcott and Richard N. Bergman, “Mortality Attributed to Covid-19 in High-Altitude Populations,” High Altitude Medicine & Biology 21, no. 4 (December 1, 2020): 409–16, https://doi.org/10.1089/ham.2020.0098.
Carson Bridgman et al., “Revisiting the Covid-19 Fatality Rate and Altitude Association through a Comprehensive Analysis,” Scientific Reports 12, no. 1 (October 27, 2022), https://doi.org/10.1038/s41598-022-21787-z.
I attended the 23rd International Hypoxia Symposium in Lake Louise, Canada to present some of the research on altitude I’ve been conducting in Colorado. The conference has been going on since 1979, and for the past 26 years the organizers have been Robert Roach and Peter Hackett, world-renowned medical researchers from Colorado. Meeting most of the famous altitude researchers from all over the world was an inspiration. Personal talks and sharing information were equally important to imbibing the latest knowledge about hypoxia and hemoglobin.
From Jay Storz’s presentation at the 2025 International Hypoxia Symposia in Lake Louise, Canada
Antarctic Icefish: Life Without Hemoglobin, was presented by Kristen O’Brien, expanding the concept of oxygen distribution in living beings and introducing us to varieties of fish we have never heard of. Her talk was followed by our “Mice and Men” guy, Jay Storz (and colleague Graham Scott), who along with Jon Velotta mentioned in our blogpost on the show “This Podcast Will Kill You” collect the large eared deer mice from peaks such as Blue Sky Mountain to study adaptation to hypoxia in their labs. The talk recognized for first prize was on Altitude Headaches, including a discussion of migraines, by Andrew Charles.
Every evening there was a banquet and speaker. Astronaut Jessica Meir spent 210 days aboard the space station. She shared a wide range of challenges such as exercising without gravity, choosing a compatible crew, getting boxes of treats from home, and effects of prolonged weightlessness on your eyes and muscles.
Silvia Ulrich presented on Pulmonary Circulation of Central Asian Highlanders at the 2025 International Hypoxia Symposium at Lake Louise, Canada.
The research I would like to see duplicated in Summit County was from Kyrgyzstan, where Silvia Ulrich studied the hearts and lungs of the permanent residents at 9000 feet using the six minute walk as one of her tools. They did not score higher when studied at sea level! She ran tests for pulmonary hypertension, which could be important here.
Of course, there was a talk on Sleep Disordered Breathing (sleep apnea) by Esther Schwarz, something we pay a great deal of attention to in our own clinic in Frisco, Colorado and have several research projects on the improvement we see with supplemental oxygen. The role of mitochondria in cellular function in hypoxia was presented by Dr. Christian Arias-Reyes, a researcher at Seattle Children’s Hospital who is originally from La Páz, Bolivia. I met him at the Chronic Hypoxia conference in 2019 when he was a graduate student in Quebec and again in La Páz at this year’s conference.
Altitude experts Dr. Zubieta Calleja, Dr. Christian Arias-Reyes, Dr. Michele Samaja and Dr. Christine Ebert-Santos with colleagues of the Hypoxia Symposia in front of a pizzeria in Coroico, Bolivia.
A deep dive into how our neurons react to hypoxia in the brain by releasing nitric oxide to dilate blood vessels and preserve circulation reenforced the counseling I do here in my clinic to parents whose children have breath holding spells or babies with dips in their oxygen on home monitors. Along with all the millions of children and adults living at 12,000 feet in Bolivia, we can witness that hypoxia does not cause brain damage. (Not to be confused with anoxia, a complete lack of oxygen.)
Lastly, Nobel prize winner and fellow pediatrician Gregg Semenza spoke on research to find a blocking compound against HIF- hypoxia inducible factor, as a cure for some cancers. Gregg’s work was described in our blog on the Nobel prize being awarded to scientists working on hypoxia. HIF deserves its own blogpost! More about cancer and hypoxia at altitude from the Chronic Hypoxia Conference in La Páz.
I was selected to give my presentation, “Colorado Kids Are Smaller” to both conferences. I have been working on this for 20 years. You can read more on our blog where it is titled “Mountain Kids Are Smaller”. My goal is to get a unique growth chart for children under age two at altitude, to save parents and providers anxiety and money trying to get our kids to “be the same” as those at sea level.
The most useful tidbit of information came on the bus ride back to Calgary. Dr Heimo Mairbaurl, PhD shared that a quarter dose of acetazolamide was sufficient for his acute mountain sickness symptom prevention, 62 mg for a guy over 6 feet tall. Although there was a study on a new possible preventive treatment, prochlorperazine, done on Mount Blue Sky last fall, I still swear by the old drug formerly known as “Diamox”.
While HAPE may be a run-of-the-mill diagnosis for providers with years of experience practicing at altitude, it can be less straightforward for those who are unfamiliar with the condition. There are currently three recognized categories of HAPE. Classic HAPE (C-HAPE) occurs when someone who resides at low altitude travels to high altitude and develops pulmonary edema. Re-entry HAPE (R-HAPE) occurs when high altitude residents travel to low altitude, then return to high altitude. High-altitude resident pulmonary edema (HARPE) occurs in high altitude residents without a change in altitude. HARPE is often brought on by an upper respiratory tract infection.
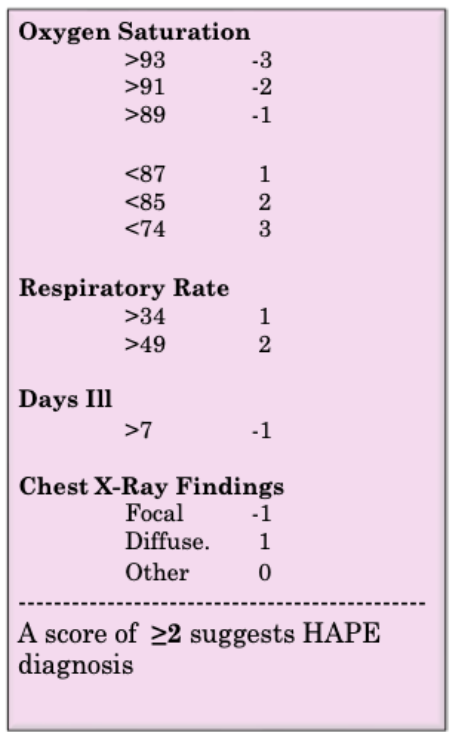
HAPE and pneumonia can have similar presentations including shortness of breath, cough, fatigue, and malaise. Patients with either condition may have decreased oxygen saturation levels and abnormal findings on chest radiography. In response to this phenomena, Dr. Chris Ebert-Santos of Ebert Family Clinic in Frisco, Colorado (9000′) and Sean Finnegan, PA-C set out to develop a scoring system to differentiate the two diagnoses. If providers could easily differentiate between pneumonia and HAPE, this would shorten the time from presentation to diagnosis and would avoid unnecessary antibiotic use.
Dr. Chris and Sean Finnegan, PA-C summarized their research findings into a scoring system named the “Frisco Score”. They analyzed data from St. Anthony Summit Medical Center and associated clinics at or above ~2,760 meters above sea level from January 1, 2018 to May 30, 2023. The study looked at patients under the age of 19 who presented with hypoxemia or other respiratory concerns and had a chest x-ray performed and oxygen saturation measured. The final case review consisted of 138 total patients with 77 diagnosed with HAPE, 38 diagnosed with pneumonia, and 23 diagnosed with concomitant HAPE and pneumonia. Variables found to have no significance included gender, age, heart rate, and temperature. Variables with significance included respiratory rate, number of days ill, oxygen saturation, and chest x-ray findings. These significant variables were used to develop the Frisco Score. They do include a disclaimer that these findings are preliminary results on a small data set. Thus, as of yet, the Frisco Score should not be used on its own to make a diagnosis, but rather should be used as a clinical tool in differentiating conditions with similar presentations.
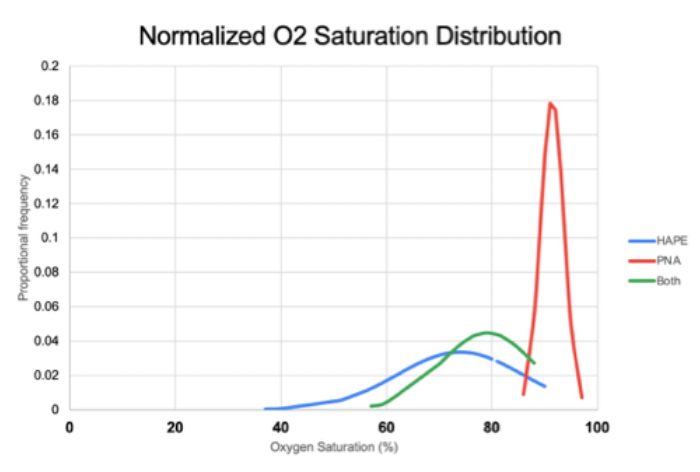
Oxygen saturation varied greatly between patients with HAPE and those with pneumonia. Patients diagnosed with HAPE had an average oxygen saturation of 74% and those with pneumonia had an average of 92%.
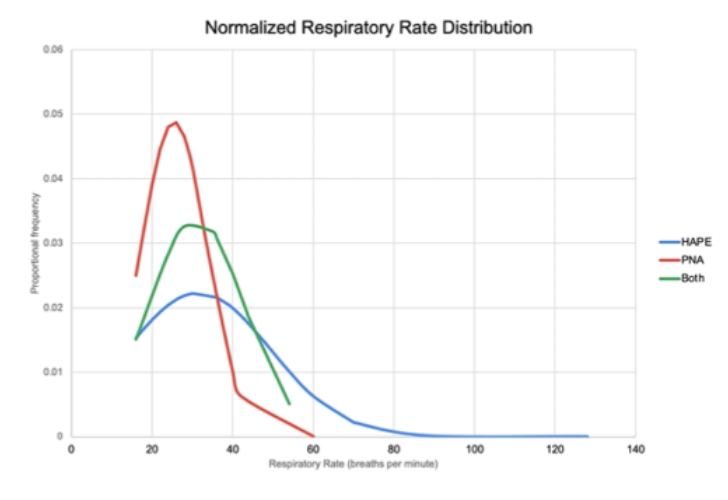
Patients who were diagnosed with HAPE had a higher average respiratory rate compared to those diagnosed with pneumonia.
In patients diagnosed with HAPE, the duration of illness, or number of days ill, was shorter than those diagnosed with pneumonia.
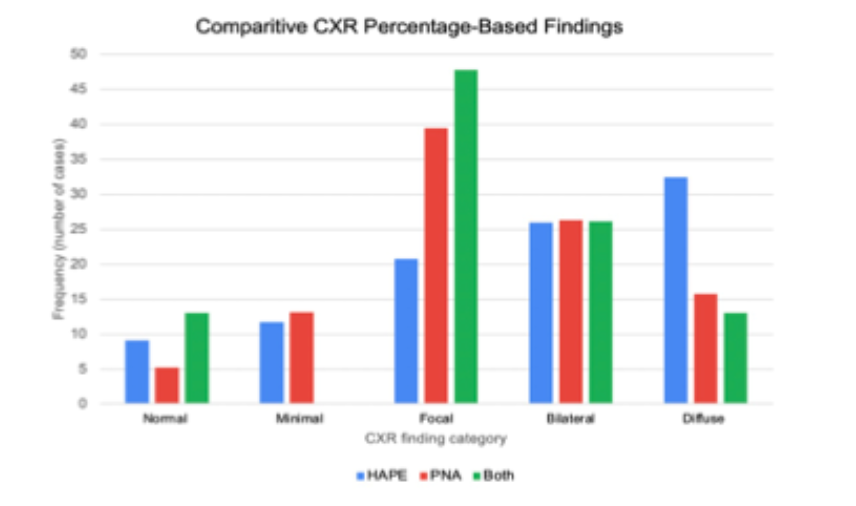
In comparison of chest x-rays, patients with HAPE were more likely to have diffuse findings and patients with pneumonia were more likely to have focal findings.
Overall, there were no variables associated with a concomitant diagnosis of pneumonia and HAPE.
In summary, patients diagnosed with HAPE had decreased oxygen saturation, increased respiratory rate, and diffuse findings on chest x-ray; while patients diagnosed with pneumonia had a longer duration of illness and focal findings on chest x-ray. The Frisco Score takes these variables into account to help differentiate a diagnosis of HAPE in children. Dr. Chris and Sean Finnegan, PA-C are currently presenting their findings at the 8th World Congress on Mountain and Wilderness Medicine in Snowbird, Utah. They hope that in the near future, the Frisco Score will be used to facilitate the diagnosis of HAPE by providers in high altitude communities state-wide.
References
1. Ebert-Santos, C. (2017). High-Altitude Pulmonary Edema in Mountain Community Residents. High Altitude Medicine & Biology, 18 (3), 278-284. https://doi.org/10.1089/ham.2016.0100
2. Ebert-Santos, C., Finnegan, S. (2024). Differentiating Pneumonia & HAPE in Children.
Founder of Ebert Family Clinic in Frisco, Colorado at 9000′, Christine Ebert-Santos, MD, MPS spent a part of her Spring 2024 backpacking across Norway:
At 2,469m (8,100 feet), Galdhøpiggen mountain in Norway is not high enough to cause altitude sickness for most people. The 300 mountain peaks over 2000m make Norway a popular destination for downhill skiing and snowboarding, as well as Nordic skiing. The long days of sunshine at this latitude allow skiing in swimsuits and summer clothes in the spring.
Norway also has the largest glacier in Europe, Jostedalsbreem. Briksdalbreen is a finger of this glacier that is a short hike in the Jostedalsbreem National Park. There are 1,600 glaciers covering one percent of Norway. Several have resorts advertising summer skiing for the whole family.
There are 900 tunnels in Norway, including the longest tunnel in the world. Compared to Eisenhower Tunnel in Colorado at 11,112 feet elevation and 1.67 miles long, Laerdal tunnel, opened in 2000, is 15 miles long with pullouts featuring colored lighting to imitate the sunrise. Some of these tunnels, like the one between the airport and downtown Oslo, go as deep as 958 feet underwater. All have phones and excellent cell phone reception. In fact, we experienced excellent reception everywhere in Norway despite the mountains and tunnels, in contrast to my sister’s house in Centennial, Colorado and many parts of Colorado.
Our last night in Norway was special. We drove two hours over narrow roads, through tunnels, over one lane bridges to Ronde Island. With a population of 150, the island is a famous bird sanctuary. We arrived just in time to see the puffins return to their nests at 8 pm. These colorful birds spend their lifespan of 30-40 years flying over the ocean, sleeping on the waves, returning to land once a year with the same mate.
The fact that Norway provides such amazing access to even this tiny town tells me how much they respect individuals. They have an average lifespan of 83 years (76 years in the USA), universal health care, one year paid leave for parents with a new baby, universal pensions, free education through college, daycare for less than $15/day, and much more. How much do they pay in taxes, you might ask? Less than what we pay when you consider the cost of health insurance, day care, school loans, with 60% of Americans who do not have anything saved for retirement.
Can I ever return to high altitude? Do I need to move down to a lower elevation?
Disease processes often differ at high altitudes. Some conditions have only been known to occur at high elevations. Most of the resources cited in this blog refer to ‘high altitude’ being at or above 2,500 meters or 8,200 feet.
Ebert Family Clinic in Frisco, Colorado is at 9,075 ft. Many areas in the immediate vicinity are over 10,000′, with some patients living above 11,000′. Two of the more common conditions seen in patients at Ebert Family Clinic are high altitude pulmonary edema (HAPE) and high altitude resident pulmonary edema (HARPE), similar conditions that affect slightly different populations in this region of the Colorado Rocky Mountains.
In “classic” HAPE, a visitor may come from a low-altitude area to Frisco on a trip to ski with friends. On the first or second day, the person notices a nagging cough. They might wonder if they caught a virus on the plane ride to Denver. The cough is usually followed by shortness of breath that begins to make daily tasks overwhelmingly difficult. One of the dangerous aspects of HAPE is a gradual onset leading patients to believe their symptoms are caused by something else. A similar phenomenon is seen in re-entry HAPE, where a resident of a high altitude location travels to low altitude for a trip and upon return experiences these same symptoms [1].
In HARPE, a person living and working here in Frisco may be getting ill or slowly recovering from a viral illness and notices a worsening cough and fatigue. These cases are even more insidious, going unrecognized, and so treatment is sought very late. Dr. Christine Ebert-Santos and her team at Ebert Family Clinic hypothesize that while residents have adequately acclimated to the high-altitude environment, the additional lowering of blood oxygen due to a respiratory illness with inflammation may be the inciting event in these cases.
In both cases, symptoms are difficult to confidently identify as a serious illness versus an upper respiratory infection, or simply difficulty adjusting to altitude. For this reason, Dr. Chris recommends that everyone staying overnight at high altitude obtain a pulse oximeter. Many people became familiar with the use of these instruments during the COVID-19 pandemic. The pulse oximeter measures what percent of your blood is carrying oxygen. At high altitude, a healthy level of oxygenation is typically ≥90%. This is an easy way to both identify potential HAPE/HARPE, as well as reassure patients they are safely coping with the high-altitude environment [2].
HAPE and HARPE are both a direct result of hypobaric hypoxia, a lack of oxygen availability at altitude due to decreased atmospheric pressures. At certain levels of hypoxia, we observe a breakdown in the walls between blood vessels and the structures in lungs responsible for oxygenating blood. The process is still not totally understood, but some causes of this breakdown include an inadequate increase in breathing rates, reduced blood delivered to the lungs, reduced fluid being cleared from the lungs, and excessive constriction of blood vessels throughout the body. These processes cause fluid accumulation throughout the lungs in the areas responsible for gas exchange making it harder to oxygenate the blood [3].
We do know that genetics play a significant role in a person’s risk of developing HAPE/HARPE. Studies have proposed many different genes that may contribute, but research has not, so far, given healthcare providers a clear picture of which patients are most at-risk. Studies have shown that those at higher risk of pulmonary hypertension (high blood pressure in the blood vessels of your lungs), are more likely to develop HAPE [4]. This includes some types of congenital heart defects [5,6]. High blood pressures in the lungs reach a tipping point and appear to be the first event in this process. However, while elevated blood pressures in the lungs are essential for HAPE/HARPE, this by itself, does not cause the condition. The other ingredient necessary for HAPE/HARPE to develop is uneven tightening of the blood vessels in the lungs. When blood vessels are constricted locally, the blood flow is shifted mainly to the more open vessels, and this is where we primarily see fluid leakage. As the blood-oxygen barrier is broken down in these areas, we may also see hemorrhage in the air sacs of the lungs [3].
One observation healthcare providers and scientists have observed is that HAPE/HARPE can be rapidly reversed by either descending from altitude or using supplemental oxygen. Both strategies increase the availability of oxygen in the lungs, reducing the pressure on the lungs’ blood vessels by vasodilation, quickly improving the integrity of the blood-oxygen barrier.
In a preliminary review of over 100 cases of emergency room patients in Frisco diagnosed with hypoxemia (low blood oxygen content) Dr. Chris and her team have begun to see trends that suggest the availability of at-home oxygen markedly reduces the risk of a trip to the hospital. This demonstrates that patients with both at-home pulse oximeters and supplemental oxygen have the capability to notice possible symptoms of HAPE, assess their blood oxygen content, and apply supplemental oxygen if needed. This stops the development of HAPE/HARPE before damage is done in the lungs. In the case of many of our patients, these at-home supplies prevent emergencies and allow patients time to schedule an appointment with their primary care provider to better evaluate symptoms.
Additionally, Dr. Chris and her team have observed that patients with histories of asthma, cancer, pneumonia, and previous HAPE/HARPE are often better educated and alert to these early signs of hypoxia and begin treatment earlier on in the course of HAPE/HARPE, reducing the relative incidence identified by medical facilities. There are many reasons to seek emergent care such as low oxygen with a fever. Patients with other existing diseases causing chronically low oxygen such as chronic lung disease may not be appropriately treated with supplemental oxygen, although this is a very small portion of the population. Discussions with healthcare providers on the appropriate prevention plan for each patient will help educate and prevent emergency care visits in both residents and visitors.
Studies of larger populations have yet to be published. A review of the case reports in smaller populations suggests that the previously estimated recurrence rate of 60-80% is exaggerated. This is a significant finding as healthcare providers have relied on this recurrence rate to make recommendations to their patients who have been diagnosed with HAPE. A review of 21 cases of children in Colorado diagnosed with HAPE reported that 42% experienced at least one recurrence [7]. This study was conducted by voluntary completion of a survey by the patients (or their families) which could lead to significant participation bias affecting the results. Patients more impacted by HAPE are more likely to complete these surveys. Another study looking at three cases of gradual re-ascent following an uncomplicated HAPE diagnosis showed no evidence of recurrence. The paper also suggested there may be some remodeling of the lung anatomy after an episode of HAPE that helps protect a patient from reoccurrence [8]. Similar suggestions of remodeling have been proposed through evidence of altitude being a protective factor in preventing death as demonstrated by fatality reports from COVID-19[9].
A review article from 2022 by Ucros et al showed a recurrence rate of 21%, high among mountain residents who travel to lower altitudes and develop reentry HAPE. An ongoing analysis of 248 hypoxic children seen in the emergency department in Frisco, Colorado at 9,000 feet found a recurrence of around 40%, again mostly reentry HAPE and HARPE, since residents have a much higher exposure to the hypoxic environment adding to their risk. Rick for visitors with classic HAPE is difficult to determine, as they are unlike to be seen in the same medical facility, but the medical history taken during the encounters in this study do not reflect any recurrence.
Without larger studies and selection of participants to eliminate other variables like preexisting diseases, we are left to speculate on the true rate of reoccurrence based on the limited information we have. Strategies to reduce the risk of HAPE/HARPE such as access to supplemental oxygen, pulse oximeters, and prescription medications [10] are the best way to prevent HAPE/HARPE. Research should also continue to seek evidence of individuals most at risk for developing HAPE/HARPE [11].
Taylor Kligerman is a third-year medical student at Rocky Vista University with plans to complete a residency in emergency medicine. She was born and raised in Flossmoor, IL, and became interested in medicine following her first medical mission trip to Gonaïves, Haiti in 2010. Taylor has extensive experience in wilderness and remote emergency medicine. Before starting medical school, she was certified as a wilderness EMT and gained experience in remote areas of Canada and Western North Carolina on whitewater expeditions and as a volunteer with local search and rescue. Her personal interests include camping, skiing, and all paddle sports.
References
Ucrós S, Aparicio C, Castro-Rodriguez JA, Ivy D. High altitude pulmonary edema in children: A systematic review. Pediatr Pulmonol. 2023;58(4):1059-1067. doi:10.1002/ppul.26294
Deweber K, Scorza K. Return to activity at altitude after high-altitude illness. Sports Health. 2010;2(4):291-300. doi:10.1177/1941738110373065
Bärtsch P. High altitude pulmonary edema. Med Sci Sports Exerc. 1999;31(1 Suppl):S23-S27. doi:10.1097/00005768-199901001-00004
Eichstaedt C, Benjamin N, Grünig E. Genetics of pulmonary hypertension and high-altitude pulmonary edema. J Appl Physiol. 2020;128:1432
Das BB, Wolfe RR, Chan K, Larsen GL, Reeves JT, Ivy D. High-Altitude Pulmonary Edema in Children with Underlying Cardiopulmonary Disorders and Pulmonary Hypertension Living at Altitude. Arch Pediatr Adolesc Med. 2004;158(12):1170–1176. doi:10.1001/archpedi.158.12.1170
Liptzin DR, Abman SH, Giesenhagen A, Ivy DD. An Approach to Children with Pulmonary Edema at High Altitude. High Alt Med Biol. 2018;19(1):91-98. doi:10.1089/ham.2017.0096
Kelly TD, Meier M, Weinman JP, Ivy D, Brinton JT, Liptzin DR. High-Altitude Pulmonary Edema in Colorado Children: A Cross-Sectional Survey and Retrospective Review. High Alt Med Biol. 2022;23(2):119-124. doi:10.1089/ham.2021.0121
Litch JA, Bishop RA. Reascent following resolution of high altitude pulmonary edema (HAPE). High Alt Med Biol. 2001;2(1):53-55. doi:10.1089/152702901750067927
Gerken J, Zapata D, Kuivinen D, Zapata I. Comorbidities, sociodemographic factors, and determinants of health on COVID-19 fatalities in the United States. Front Public Health. 2022;10:993662. Published 2022 Nov 3. doi:10.3389/fpubh.2022.993662
Luks A, Swenson E, Bärtsch P. Acute high-altitude sickness. European Respiratory Review. 2017;26: 160096; DOI: 10.1183/16000617.0096-2016
Dehnert C, Grünig E, Mereles D, von Lennep N, Bärtsch P. Identification of individuals susceptible to high-altitude pulmonary oedema at low altitude. European Respiratory Journal 2005;25(3):545-551; DOI: 10.1183/09031936.05.00070404
Hypoxia is a common presentation at the emergency department for the St Anthony Summit Medical Center, located at 2800 meters above sea level (msl) in Colorado. Children under 18 are brought in with respiratory symptoms, trauma, congenital heart and lung abnormalities, and high altitude pulmonary edema (HAPE). Many complain of shortness of breath and/or cough and are found to be hypoxic, defined as an oxygen saturation below 89% on room air for this elevation. Patients who live at altitude may perform home pulse oximetry and arrive for treatment and diagnosis of known hypoxia. Extensive and ongoing analysis of the data from children found to be hypoxic in the emergency department raises many questions, including how residents vs nonresidents present, how often these cases are preceded by febrile illness and what chief complaint is most frequently cited.
Understanding the presentation of hypoxia in children at altitude can help ensure that healthcare providers are following a comprehensive approach with awareness of the overlapping symptoms of HAPE, pneumonia and asthma. Below is a graphic summary of 36 cases illustrating the clinical, social and geographic factors contributing to hypoxia at altitude in residents and visitors. A further analysis of over 200 children with hypoxia presenting to the emergency room at 9000 feet is underway including x-ray findings.
The graphs below were created by the author, using data extracted directly from a review of patient charts (specifically, those of children presenting to the local hospital in Summit County, Colorado (9000 feet) with hypoxia).
Graphs 1-4 show chief complaints of cough (CC) and shortness of breath (SOB) compared by age and by residence (res: includes altitudes above 2100 meters above sea level), the front range (a high altitude region of the Rocky Mountains running north-south between Casper, Wyoming and Pueblo, Colorado) averaging 1500 msl, and out of the state of Colorado (OOS).
Graphs 9 and 10 show lowest oxygen by age at admission and lowest O2 organized by days spent in the county (residents are excluded from this data).
Erin Snyder is a new graduate physician assistant who graduated this fall after spending her final rotation in Frisco with the Ebert clinic. She is now working in pediatric hematology at Children’s Hospital Colorado. And her free time she enjoys skiing, hiking and spending time with her cat Charlie.
Emergency medicine physician at Aspen Valley Hospital and medical director for Mountain Rescue Aspen since 1997 Dr. Scott A. Gallagher2 and emergency physician and altitude research pioneer Dr. Peter Hackett3 introduce the resource warning, “Anyone who travels to high altitude, whether a recreational hiker, skier, mountain climber, soldier, or worker, is at risk of developing high-altitude illness.”
Ebert-Santos’s (known affectionately to her patients and mountain community as “Dr. Chris”) own research is referenced in the article’s discussion of epidemiology and risk factors noting an additional category of HAPE among “children living at altitude who develop pulmonary edema with respiratory infection but without change in altitude,”4 whereas the two other recognized categories (classic HAPE and re-entry HAPE) typically happen in response to a change in altitude.
The article continues with figures illustrating how ascending too quickly or too much can dramatically increase risk: “HAPE generally occurs above 2500 meters (8000 feet) and is uncommon below 3000 meters (10,000 feet) … The risk depends upon individual susceptibility, altitude attained, rate of ascent, and time spent at high altitude. in those without a history of HAPE, the incidence is 0.2 percent with ascent to 4500 meters (14,800 feet) over four days but 6 percept when ascent occurs over one to two days. In those with a history of HAPE, recurrence is 60 percent with an ascent to 4500 meters over two days. At 5500 meters (18,000 feet), the incidence ranges between 2 and 15 percent, again depending upon rate of ascent.”
“‘The first sign is usually a cough,’ Ebert-Santos said. ‘Followed by shortness of breath with any effort — even just walking — and fatigue. You just want to lie on the couch.’
If left untreated the early warning signs of high altitude pulmonary edema can rapidly progress into having fluid build up in the lungs, which will then lead to a patient’s oxygen saturation levels rapidly decreasing. If the individual does not seek treatment quickly, the condition can be fatal.”